Archive for September 2007
Health Care Data Cleaning becomes Big Business
The WSJ blog details how Athenahealth is hoping to earn profits by helping doctors comply with arcane insurance company, Medicaid, and Medicare data processing requirements. They present this as entirely wasteful. It’s not. If, like all health policy wonks and politicians, you want analytically useful healthcare data, someone has to force data compliance at the point of service. This means burdening doctors. How else will you get data on disease management practices and effectiveness? Or to evaluate physician quality? (note: all insurance companies are being required to do this)
Clean data is incredibly expensive.
Since the movement for clean analytic data began, Medicare, Medicaid and insurance companies have built claim systems to make sure that submitted claims have sensible diagnostic and procedure codes associated with them. If the claims are unusual, they will generally deny in part or in total and, at a minimum, force a manual review process. This ensures a minimum standard of cleanliness in the data. This, in turn, forces doctors to increase their data sophistication.
Is all of this effort worth the cost? I have no idea; but we shouldn’t pretend that we aren’t buying something with all of this money spent on IT. You can’t simultaneously argue that this administration expenditure is worthless while at the same time demanding that people engage in ever-more-detailed disease management, wellness programs, or even purely academic analyses.
Concord Coalition on SCHIP
I just ran across this excellent Concord Coalition analysis of SCHIP funding proposals. They brought new information to bear on two points.
First, the funding for SCHIP runs for 5 years, after which it “sunsets” and has to be reappropriated. Unlike the CC, I don’t view this as a bad thing. However, this version is additionally cynical because it provides for a one-time special appropriation in 2012. This appropriation is not scored as an expenditure by the CBO.
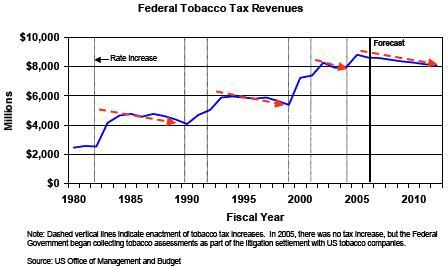
Second, the use of the cigarette tax to raise offsetting revenue is an especially poor vehicle. SCHIP expenses are likely to increase faster than the rate of inflation and for as long as the eye can see. Cigarette taxes will fund the program. But as their graphic (reproduced below) illustrates, cigarette tax revenue tends to decline over time, not increase.
Combined, these two political gimmicks suggest that the bill builds in unfortunate long-term funding imbalances.
Smoking and low income status are correlated. Therefore, this bill brings up an additional oddity. It taxes the poor in order to give the poor some financial protection. A noble sacrifice.
Selective Perspectives on Fiscal Responsibility
Econbrowser‘s Menzie Chinn writes critically on the sudden and arguably selective fiscal restraint of the Bush II administration. Chinn argues that a $5 billion per year SCHIP expansion is small potatoes compared to Part D and other fiscal ills of the current administration.
Relatively speaking, I agree. However, he mixes and matches time horizons, thereby making his suggested comparison flawed.
David Walker from the GAO has been on a Fiscal Wake-up Tour. Here’s his latest chart.

Notice that the implicit exposures are actually the present values of 75-year liabilities. For example, the Medicare Part A liability of $11.3 trillion comes from the 2006 Medicare Trustee Report (Table III.B9).
On a 75-year present-value basis, what is a better estimate for the cost of SCHIP expansion? My quick answer is $439 billion. This would be the apples-to-apples comparison. This is still dwarfed by the size of Part D. However, it is also not small potatoes, to mix my fruit metaphors.
Lastly, although all of these numbers are shockingly large, it is important to remember that they may occur over a very long period of time. The collective resources available to the American economy over the next 75 years are likewise immense. Therefore, perhaps the best practice is not to mix 75-year cost projections into the SCHIP argument at all.
Regardless, if anyone wants more details on my calculations and assumptions, see below the fold.
Read the rest of this entry »
ESRD: A Case Study in Single Payer Health Insurance
Medicare’s struggles with End-Stage Renal Disease (ESRD) provide insight into government provided healthcare. In 1972, President Nixon signed a bill that provided universal coverage for all Americans who have ESRD. At the time, there were 7,000 people with ESRD on dialysis. It seemed a managable socialization.
Now, we have more than 300,000. In 2002, ESRD represented more than 6.7% of all Medicare expenditures. We have discovered new drug treatments like Epogen which help fights anemia for those on dialysis. Government payment structures have lagged technology. From 1983 to 2003, when the infamous Medicare Modernization Act was passed, government paid providers for a bundle of services via something known as a composite fee. Now, we are trying to do something about it.
There is a war on for how to pay for ESRD treatments. This WSJ article ($$) details the complex political issues involved. One way to trim costs is to eliminate “overprescription” of Epogen, which may ultimately be harmful for those receiving the higher doses. But what is overprescription? It turns out that African Americans receive more Epogen, perhaps because of a higher incidence of related complications. So far, Congressional Democrats have been undeterred in their attempt to save money by limiting Epogen prescriptions. However, the racial overtones of these decisions are now being looked at, and the Congressional Black Caucus may be break with Democrats, stalling funding reform. We’ll see.
The politicization of medicine is just one of the problems we are facing with ESRD. The government’s virtual monopoly on ESRD treatments plays havoc with traditional government methods for determining fair levels of remuneration. This is especially true for valuing a drug like Epogen. Bruce Steinwald’s GAO congressional testimony described the impact of the current method, which takes the Average Sales Price (ASP) from the manufacturer and arbitrarily adds 6%:
… certain unknowns about the composition of ASP and the ASP-based payment formula make it difficult for CMS to determine whether the ASP-based payment rates are no greater than necessary to achieve appropriate beneficiary access. For one thing, CMS has no procedures for validating the accuracy of a manufacturer’s ASP, which is computed by the manufacturer. For another, CMS has no empirical justification for the 6 percent add-on to ASP. Regardless of how payment for these drugs is calculated, as long as facilities receive a separate payment for each administration of each drug and the payment exceeds the cost of acquiring the drug, an incentive remains to use more of these drugs than necessary.
…
Epogen is the only product available in the domestic ESRD market for anemia management. However, the ASP method relies on market forces to achieve a favorable rate for Medicare. When a product is available through only one manufacturer, Medicare’s ASP rate lacks the moderating influence of competition. The lack of price competition may be financially insignificant for noncompetitive products that are rarely used, but for Epogen, which is pervasively and frequently used, the lack of price competition could be having a considerable adverse effect on Medicare spending.
The result: two billion dollars spent on Epogen per year, and a lot of chaos.
Flour Flyer Followups
The New Haven Register is continuing to follow the story of the now-infamous flour flyer. From the links at the end of this post, we can now compile this timeline.
Read the rest of this entry »
